60 year male with heart failure
roll no: 55
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
Following is the view of my case:
60yr old male labourer by occupation came with the complaints of cough with expectoration since 10days
Breathless since 10days
Patient was apparently alright 10days ago then he developed cough with expectoration since 10days, insidious in onset, gradually progressive in nature, present during night time, sputum- white in colour, scanty, non foul smelling, non blood stained
Breathlessness since 10days, insidious onset, Gradually progressive in nature, needs to stop for breath when walking at own pace
(grade II MMRC) Aggravated on exertion, relieved on rest
H/o chest pain while coughing, orthopnea and PND present, sleep disturbed
No h/o profuse sweating, pedal oedema
Constipation present since 5years- passes stool once in 2days, hard stools, non blood stained
Urinary hesitancy present since 5years
No h/o similar complaints in the past
Not a known case Type 2 DM, HTN,CVA,CAD,TB,Asthma
Personal history -
Appetite : normal
Diet: mixed
Bowel and bladder: regular
Sleep: adequate
Addictions:smokes cigarettes 4-5 per day since 40years
Occasional alcoholic for 5years, stopped since 1 year
General examination:
No pallor, icterus, cyanosis, clubbing, lymphadenopathy, oedema of foot.




Vitals:
Bp:110/8mmhg
PR:87bpm
Rr:20cpm
SpO2-98 on RA
CVS- s1s2 heard; no murmurs
RS- Bilateral air entry present
Wheeze present in right infraclavicular ; right mammary and axillary areas
PA- soft non tender
CNS- higher mental functions intact
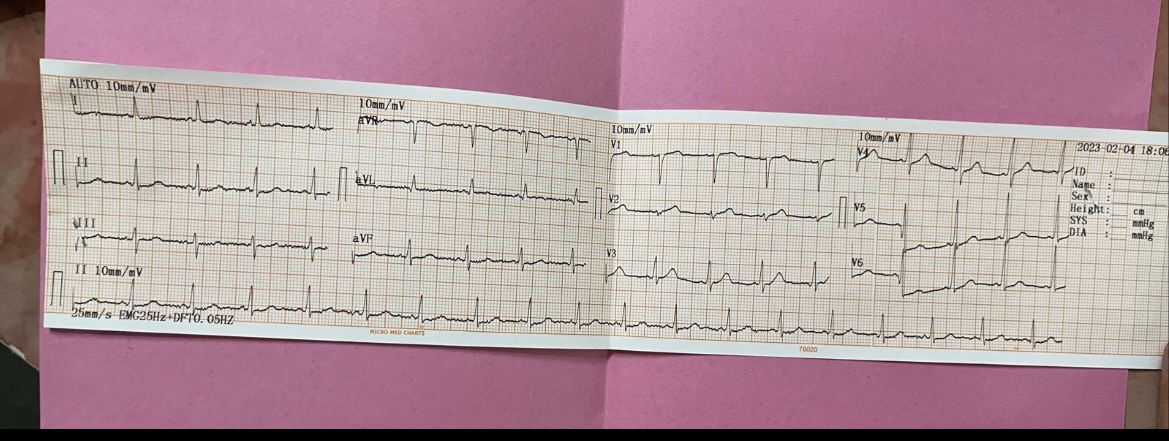
Investigations:
Ecg
Nebulisation with budecort and duolin 6th hourly
Tab ECOSPRIN AV 75 /10 mg po h/s
Tab PAN 40 mg PO/ OD
Tab DYTOR 10 mg PO / BD
Tab MET-XL 25 mg PO/OD
Tab TELMA 40 mg PO / OD
Syp CREMAFFIN PLUS 15 ml PO/ H/S
Inj OPTINEURON in 100ml NS / OD
7/2/23
HB: 14.2
TLC:13,000
RBC: 5.15
PLT:3.49
Sr. Calcium: 9.8
Phosphorus:2.6
Sodium: 129
Potassium: 4.1
Chloride: 92
Calcium ionized: 1.12
8/2/23
Hb: 14.0
TLC: 11,000
RBC: 5.05
PLT:3.48
CUE:
Albumin:++
Pus cells: 4-6
Epithelial cells: 1-2
Red blood cells: 6-8
A

Comments
Post a Comment